

One in five adults in the United States lives with a mental health condition. In Texas, the odds of getting treatment for that condition are among the worst in the country.
According to Mental Health America’s 2025 State of Mental Health in America report, Texas ranks 46th in the nation for mental health care access a position it has held for multiple consecutive years. More than 5 million Texas adults experience a mental illness annually. Over 54% of them receive no treatment at all.
That’s not a funding gap. That’s not a staffing shortage. That is a system failure and it is measurable, documentable, and getting worse as Texas’s population grows.
But in Austin, one clinic is operating with a fundamentally different model. And it’s working.
The Texas Mental Health Crisis: What the 2025–2026 Data Shows
The numbers behind Texas’s ranking are worth sitting with:
- 46th nationally for overall mental health care access (Mental Health America, 2025)
- Texas has roughly 1 psychiatrist per 4,500 residents far below the national recommended ratio
- $39 per capita Texas’s state mental health spending, one of the lowest in the nation (NAMI Texas, 2025)
- 56 of 254 Texas counties have zero mental health providers of any kind
- Among Texas adults with serious mental illness, less than 40% receive minimally adequate treatment
The COVID-19 pandemic accelerated these trends. The 2021 freeze, ongoing housing instability in Austin, and the economic pressure of one of the fastest-growing metros in the country have compounded mental health strain across every demographic from young professionals to college students to families managing multiple stressors simultaneously.
Austin is not immune. In fact, the city’s rapid growth has created its own specific pressures: housing costs that rose over 40% between 2020 and 2024, social isolation in sprawling new developments, and a tech-sector culture that rewards performance and penalizes vulnerability.
Why Most People Don’t Get Help
The access problem is not simply a matter of availability. Even in cities with mental health providers, the barriers are real and varied:
Cost. Outpatient therapy in Austin averages $150–$250 per session out of pocket. Many providers don’t take insurance.
Wait times. The average wait for a new psychiatry appointment in Texas is 25 weeks more than six months.
Stigma. Among Texans with mental health conditions, stigma remains one of the top reported barriers to seeking care particularly in professional, religious, and military-connected communities.
Complexity. Navigating insurance panels, step-down levels of care, and the difference between a therapist, psychiatrist, and case manager is genuinely confusing and the burden of figuring it out falls entirely on the person who is already struggling.
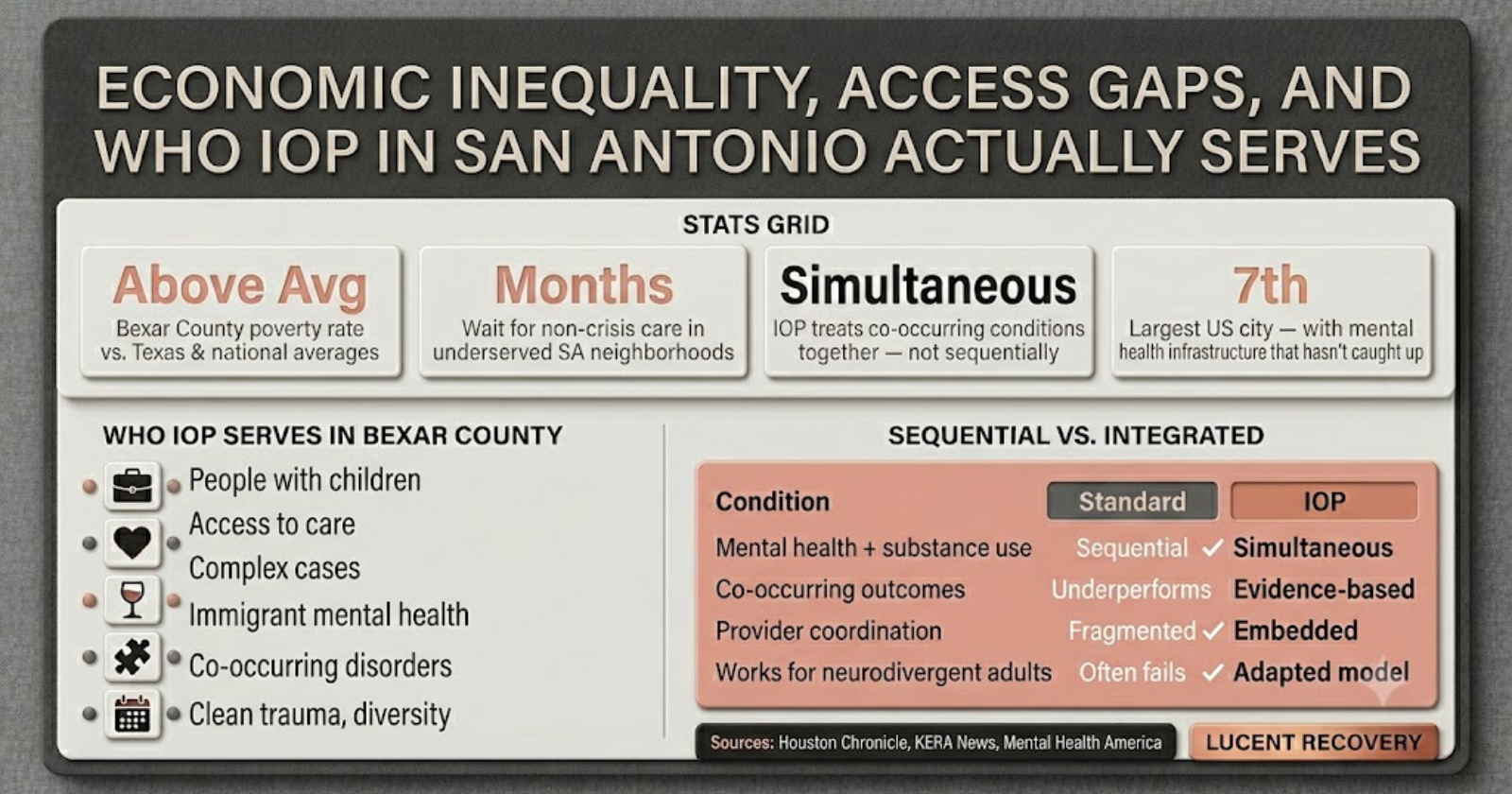
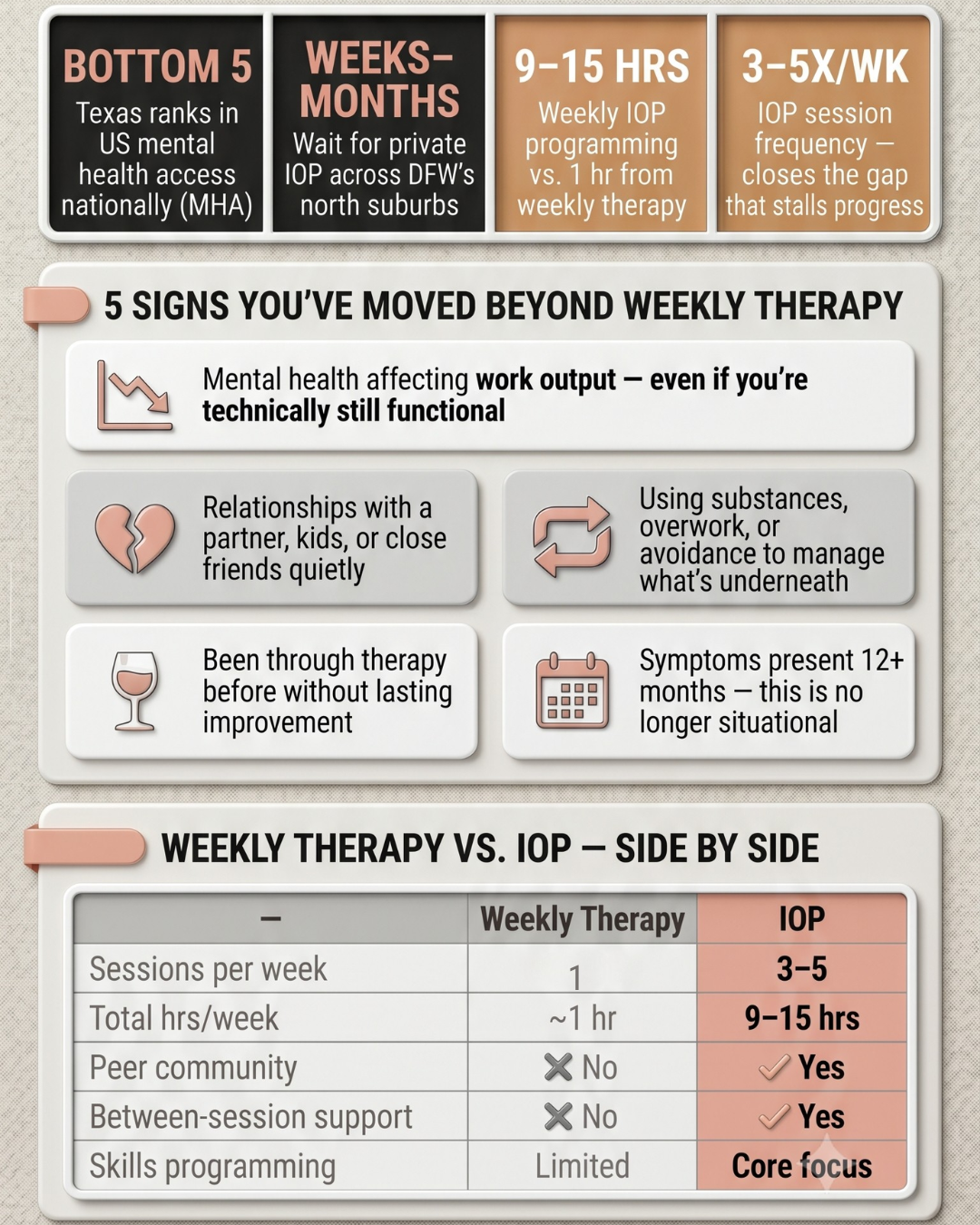
Gaps between care levels. Texas has inpatient psychiatric facilities. It has private therapists. What it lacks is a robust middle layer the intensive outpatient and partial hospitalization programs that serve people who need more than weekly therapy but don’t need hospitalization.
That middle layer is exactly where Lucent Recovery and Wellness operates.
What Lucent Recovery and Wellness Actually Does
Lucent Recovery and Wellness is a clinician-owned outpatient mental health treatment center in Austin. Founded in 2020, it was built specifically to fill the gap in the Texas care continuum to be the kind of place that treats people with the seriousness and warmth their conditions require.
This is not a drop-in counseling center. Lucent offers a structured, clinical-grade continuum of care designed around each individual client:
Intensive Outpatient Program (IOP)
Lucent’s IOP provides multiple therapy sessions per week individual, group, and skills-based while allowing clients to continue living at home, maintaining work or school, and staying connected to their support systems. It bridges the gap between weekly therapy and full residential treatment.
Treatment modalities include:
- Cognitive Behavioral Therapy (CBT) targeting distorted thought patterns driving anxiety, depression, and emotional dysregulation
- Dialectical Behavior Therapy (DBT) building emotion regulation, distress tolerance, and interpersonal effectiveness skills
- EMDR (Eye Movement Desensitization and Reprocessing) evidence-based trauma processing
- Somatic Experiencing body-based trauma resolution
- Mindfulness-Based Stress Reduction (MBSR)
Partial Hospitalization Program (PHP)
For clients who need more structured support, Lucent’s PHP offers a higher level of clinical intensity typically 5 days per week while still maintaining outpatient status. It is the highest level of care that does not require overnight residency.
Master’s-Level Case Management
Every client at Lucent has access to case management by master’s-level clinicians who coordinate care, navigate system barriers, and provide continuity across every aspect of a client’s treatment and life situation.
Recovery Coaching and Fitness
Lucent integrates experiential recovery coaching and health and fitness programming as clinical components not add-ons. Research consistently shows that physical activity and structured goal-setting are meaningful adjuncts to mental health treatment.
Transitional Housing
For clients who need structured living support during or after treatment, Lucent’s transitional housing program provides a stable environment while intensive care continues.

What Makes Lucent Different from Standard Outpatient Care
Texas has outpatient mental health providers. What it rarely has is this:
Clinician-owned. Lucent is not a PE-backed behavioral health chain. It was founded by clinicians who still practice there. That matters for clinical quality and for the culture of care clients experience.
Low clinician-to-client ratios. Large group practices and hospital-affiliated programs often carry caseloads that make genuine individualization impossible. Lucent’s structure is designed around smaller caseloads and deeper clinical relationships.
Trauma-informed at every level. Trauma-informed care is not a checkbox at Lucent. It shapes intake, treatment planning, how sessions are structured, and how clinicians are trained. For a population where unresolved trauma underlies the majority of presenting diagnoses, this is not optional it’s the foundation.
Integrated services under one roof. Rather than requiring clients to navigate multiple providers across the city, Lucent offers therapy, case management, psychiatric coordination, coaching, and fitness support as a coherent package.
“We’ve had clients tell us this was the first time they felt like a clinician really listened. That kind of connection that’s where the healing begins.”
What Healing Actually Looks Like
The clinical outcomes speak clearly, but the human outcomes matter more. Clients who complete Lucent’s programs commonly report:
- Significant reduction in anxiety, depression, and acute emotional distress
- Improved capacity to manage relationships and regulate stress responses
- Renewed sense of purpose and personal identity
- Reconnection with family and community support systems
- Skills and strategies they use independently long after treatment ends
For many clients, Lucent represents the first time they have been able to speak about trauma, mental health, or emotional pain without shame or fear of judgment. That experience alone being genuinely seen is often the turning point.
What Needs to Change at the System Level
Lucent is one clinic. Texas’s mental health crisis requires systemic solutions:
- Increased state investment in community mental health funding (Texas currently spends less per capita than 44 other states)
- Expanded Medicaid access Texas remains one of the 10 states that has not expanded Medicaid, leaving hundreds of thousands of low-income Texans without mental health coverage
- Workforce development training and licensing pipelines for LPCs, LCSWs, and psychiatrists, with incentives for rural and underserved area practice
- Anti-stigma campaigns at the employer and community level, particularly in sectors military, oil and gas, tech where help-seeking is culturally penalized
- Expanded IOP/PHP infrastructure across the state the middle level of the care continuum where Lucent operates is the most underdeveloped and most needed
Until those changes happen, clinics like Lucent hold the line.
Frequently Asked Questions
Does Lucent accept insurance?
Lucent works with many insurance providers. Contact their team directly at 512-588-3899 to verify your specific coverage before beginning treatment.
Who is a good fit for Lucent’s IOP?
Adults experiencing moderate to significant mental health symptoms including depression, anxiety, PTSD, trauma, bipolar disorder, personality disorders, or co-occurring substance use who need more support than weekly therapy but do not require inpatient hospitalization.
What is the difference between IOP and PHP?
IOP typically involves 9–15 hours of structured treatment per week. PHP is more intensive, generally 25–30 hours per week. Both allow clients to live at home. Your intake clinician will recommend the appropriate level based on your current clinical picture.
Does Lucent offer services outside Austin?
Lucent’s primary facility is in Austin. They serve clients from across the Austin metro area, including clients who relocate temporarily to access their transitional housing program.
If You’re Ready to Take the Next Step
Texas’s mental health system is failing too many people. But that doesn’t mean you have to wait for the system to fix itself.
Lucent Recovery and Wellness is ready to help now with clinical expertise, genuine compassion, and a structure designed to meet you where you are.
📞 Call: 512-588-3899
📍 Location: 4807 Spicewood Springs Rd #1100, Austin, TX 78759
🌐 Online: lucentrecovery.com/contact-us
You don’t have to carry this alone. And you don’t have to wait six months for a psychiatry appointment to start getting real help.

Reviewed by Chris Hudson, LPC
Founder & Executive Director – Lucent Recovery and Wellness, Austin, TX (2020–Present)
Leads clinical programs and develops innovative therapeutic approaches integrating experiential and creative therapies.
Board Member – Reklaimed, Austin, TX
Supports recovery-focused nonprofit initiatives fostering community and creative skill-building.
Clinical Leadership Roles – South Meadows Recovery, Inc.
Held leadership positions overseeing program development, clinical operations, and organizational management.
EDUCATION & CREDENTIALS
- M.A., Clinical Mental Health Counseling – Seminary of the Southwest (2021)
- B.A., Studio Art – Lewis & Clark College (2004)
- Licensed Professional Counselor (LPC), Texas
- Licensed Chemical Dependency Counselor (LCDC), Texas
")












Latest posts